


On October 16, 2019, in order to further promote the implementation of the "Comprehensive Plan for the Prevention and Control of Myopia in Children and Adolescents", and to guide the scientific implementation of myopia prevention and control work for children and adolescents in various regions, the National Health Commission organized the development of the "Appropriate Technical Guidelines for the Prevention and Control of Myopia in Children and Adolescents".
Preferable Technical Guidelines for the Prevention and Control of Myopia in Children and Adolescents
Myopia in children and adolescents in China has become a focus of society due to its high incidence and younger onset, which seriously affects their physical and mental health. In order to actively implement General Secretary Xi Jinping's important instructions on the issue of myopia in children and adolescents, further promote the implementation of the Comprehensive Plan for the Prevention and Control of Myopia in Children and Adolescents, guide the scientific and standardized prevention and control work, and improve prevention and control technical abilities, the National Health Commission has formulated the "Guidelines for the Appropriate Prevention and Control of Myopia in Children and Adolescents" (hereinafter referred to as the "Guidelines").
I. Scope of Application
The "Guidelines" apply to the prevention and control of myopia in children and adolescents, and the target audience is technical personnel engaged in the prevention and control of myopia in children and adolescents at the provincial, municipal, and county levels.
II. Basic Knowledge of Myopia Prevention and Control
(A) Terminology.
1.Visual acuity: also known as sharpness of vision, refers to the ability of the eyes to identify objects, which is divided into central visual acuity and peripheral visual acuity (i.e. visual field). The former refers to the visual acuity of the fovea in the macular area of the retina, while the latter refers to the visual acuity beyond the fixation point in the macular area. Generally, the so-called visual acuity refers to central visual acuity. The ability to recognize distant objects is called distance visual acuity, while the ability to recognize nearby objects is called near visual acuity.
2.Uncorrected visual acuity: also known as unaided visual acuity, refers to the visual acuity measured without any optical correction, including uncorrected distance visual acuity and uncorrected near visual acuity.
3.Corrected visual acuity: refers to the visual acuity measured after optical correction with glasses or contact lenses, including corrected distance visual acuity and corrected near visual acuity.
4.Poor vision: also known as visual impairment, refers to a condition where the uncorrected visual acuity measured using the Standard Logarithmic Visual Acuity Chart (GB11533-2011) is less than 5.0 in children and adolescents aged 6 years or older. Among them, a visual acuity of 4.9 is mild visual impairment, 4.6≤ visual acuity ≤4.8 is moderate visual impairment, and visual acuity ≤4.5 is severe visual impairment. The causes of poor vision in children and adolescents are mostly due to refractive errors such as myopia, hyperopia, astigmatism, and other eye diseases (such as amblyopia, strabismus, etc.).
5.Myopia: refers to a pathological condition in which the human eye, in a relaxed state of accommodation, causes parallel light from 5 meters away to focus in front of the retina after passing through the eye's refractive system. Its manifestation is a decrease in distance vision.
6.Screening myopia: using fast and convenient methods such as distance vision tests, computer-assisted refraction (commonly known as computerized refraction) in a non-cycloplegic state, or retinoscopy to screen for children and adolescents who may have myopia. When the naked-eye distance vision of children and adolescents over 6 years old is less than 5.0, and the equivalent spherical power (SE) is less than -0.50D under non-cycloplegic refraction, it is judged as screening myopia; in areas equipped with computerized refractors, retinoscopy can be used, and if the positive lens (convex lens) vision is decreased, and the negative lens (concave lens) vision is improved, it is judged as screening myopia.
7.Cycloplegic refraction examination: Cycloplegic refraction, also known as dilation refraction, is the internationally recognized gold standard for diagnosing myopia. It is recommended that children under 12 years old, especially those who are being tested for the first time, or those with hyperopia, strabismus, amblyopia, and high astigmatism, must undergo cycloplegic refraction examination to diagnose myopia and those who require glasses need regular follow-up examinations.
(B) Classification of Myopia
1.Myopia can be classified into three different degrees based on the degree of equivalent spherical refractive error (SE) measured by a pupil-dilated autorefractor:
(1) Low myopia: -3.00D ≤ SE < -0.50D (between 50 and 300 degrees of myopia);
(2) Moderate myopia: -6.00D ≤ SE < -3.00D (between 300 and 600 degrees of myopia);
(3) High myopia: SE < -6.00D (over 600 degrees of myopia).
2.According to the progression and pathological changes of myopia, myopia can also be divided into simple myopia and pathological myopia.
(1) Simple myopia mostly refers to myopia developed during the eyeball's growth period, which tends to stabilize when the growth stops. The refractive error is generally within -6.00D. Most patients have no pathological changes in the fundus, and their vision can be corrected to normal with appropriate optical lenses.
(2) Pathological myopia mostly refers to myopia that continues to progress after growth stops and is accompanied by pathological changes in the fundus. It is also called progressive myopia, and the degree of myopia is mostly above -6.00D. Common fundus changes include myopic crescent, lacquer cracks, choroidal neovascularization, macular choroidal atrophy, retinal detachment, and posterior staphyloma.
(C)Symptoms and Hazards of Myopia
The typical symptom of myopia is a decrease in distance vision. The main manifestations include:
(1) Decrease in distance vision, with fluctuations in initial myopia;
(2) Involuntary squinting or tilting of the head when looking at distant objects;
(3) Uncorrected myopia can cause visual fatigue symptoms;
(4) Patients with high degrees of myopia often have poor night vision, and may experience floaters, flashes, and other symptoms. They may also have varying degrees of fundus changes. Particularly for high myopia patients, the risk of retinal detachment, tear, macular hemorrhage, neovascularization, and angle-closure glaucoma is increased, which can lead to blindness in severe cases.
III. Appropriate techniques for myopia prevention and control
(A)Screening for visual impairment and myopia
According to the "Technical Specification for Children's Eye and Vision Health" and the "National Basic Public Health Service Specification (Third Edition)", efforts should be made to provide eye health and vision examination for children aged 0-6 years old, to detect early eye diseases and high-risk factors that affect children's visual development, and to refer and treat them in a timely manner to protect and promote normal visual development in children.
Establish a regular screening system for vision among primary and secondary school students, conduct tests for visual impairment, including uncorrected visual acuity, corrected visual acuity (if wearing glasses), and non-cycloplegic refraction, and assess the factors that affect visual health. In areas with conditions, encourage the measurement of axial length and corneal curvature. The screening of distance vision should use the "GB11533-2011 International Logarithmic Visual Acuity Chart". The screening frequency should be at least once per academic year. The automatic computerized refractometer used for computerized optometry should comply with the provisions of "ISO10342-2010 Ophthalmic instruments: Refractometer".
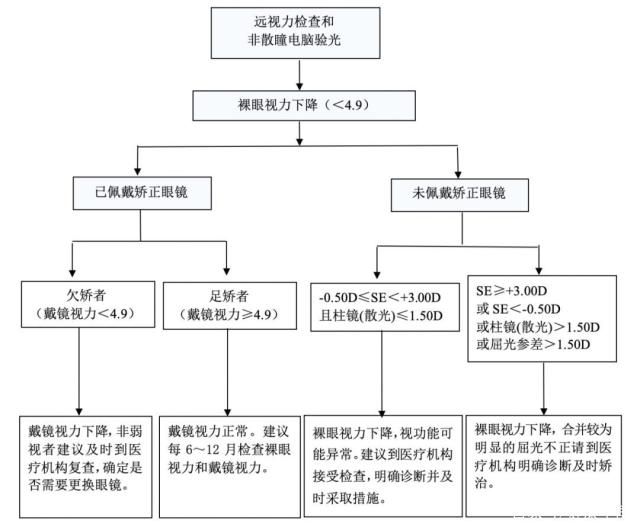
Carry out visual screening for children and adolescents in kindergartens and primary and secondary schools, and provide professional technical services and guidance. The screening unit shall provide feedback on the screening results within one month after the screening, in accordance with the screening technical process flow chart (see Figures 1 and 2), and provide precise guidance on myopia prevention or referral recommendations. Special attention should be paid to providing information feedback and eye hygiene guidance to myopic children and adolescents. For those with suspected insufficient farsightedness reserves (normal uncorrected visual acuity, although the refractive state does not reach the myopia standard, it deviates from the corresponding physiological value range for the age group) and those with high-risk factors for myopia, high-risk warnings should be given, and key interventions should be implemented. At the same time, the examination results should be fed back to the school within one month, including the time of examination, the number of people examined, and the incidence of visual impairment and screening myopia rate by grade and class, and compared with the results of the previous academic year.

(B)Establishment of Visual Health Records
Regular visual acuity examinations should be conducted for children aged 0-6 years and primary and secondary school students, and the examination contents should be recorded in accordance with the "Record Form for Children and Adolescents' Myopia Screening Results" (see Table 1) to establish visual health records for children and adolescents. In areas where conditions permit, eye appearance, eye position, eye movement, and refractive development may also be included as examination contents.
The visual health status of children and adolescents should be analyzed in a timely manner, and myopia and other refractive errors should be screened for early. Changes in refractive status during different stages of childhood and adolescence should be dynamically observed to identify the tendency or trend of myopia development and to develop intervention measures to reduce myopia, especially high myopia. Primary schools should receive visual health records, such as the "Record Form for Children and Adolescents' Visual Acuity Examination" from medical and health institutions each year, and ensure that each student has their own record file, which should be transferred in real-time with their enrollment changes, and be linked with the visual acuity examination of primary and secondary school students.
Table 1 Record of Myopia Screening Results for Children and Adolescents

(C) Cultivate healthy eye habits.
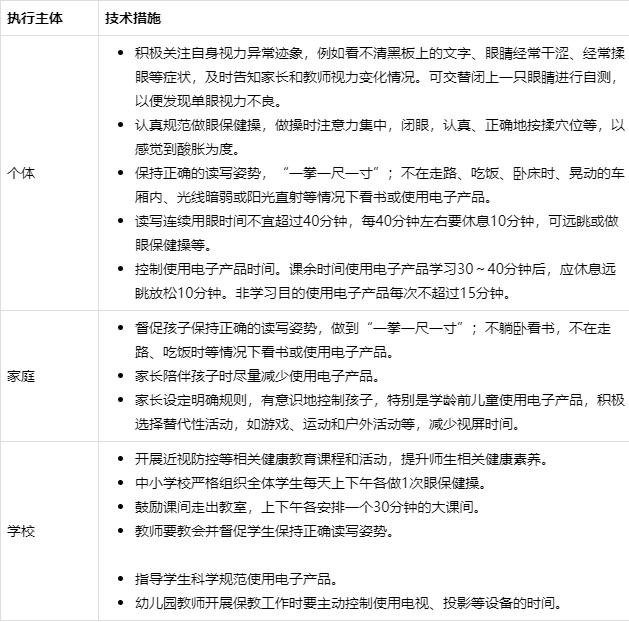
Individuals, families, and schools should actively cultivate the awareness that "everyone is responsible for their own health", actively learn and master eye health knowledge and skills; parents and guardians should understand scientific eye use and eye care knowledge, lead by example, strengthen outdoor activities and physical exercise, and reduce the academic burden on students; cultivate and supervise children and adolescents to develop good eye hygiene habits, enabling them to establish a love for their eyes and protective eye behavior.
(D) Creating a vision-friendly environment.
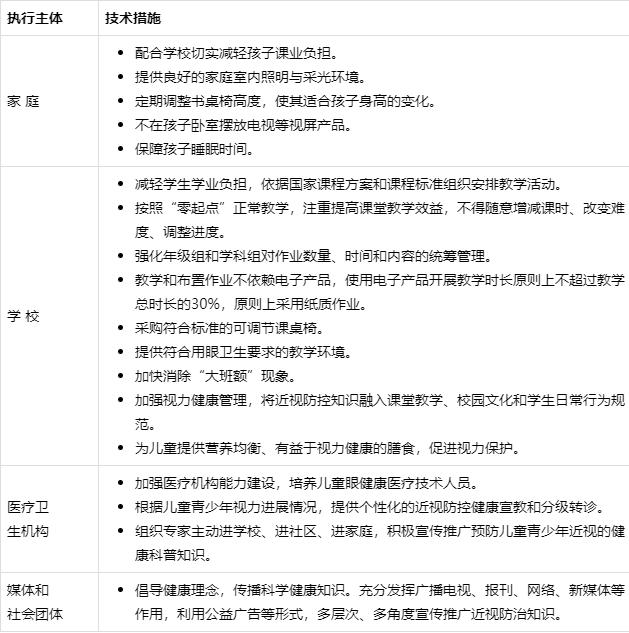
All sectors including families, schools, healthcare institutions, media, and other social groups should proactively participate in creating a vision-friendly environment. Families and schools should follow relevant national policies and standards, reduce students' academic burdens, improve lighting conditions, and provide desks and chairs suitable for children and adolescents' height. The media and community should increase the promotion of relevant standards and knowledge and create a supportive social environment.
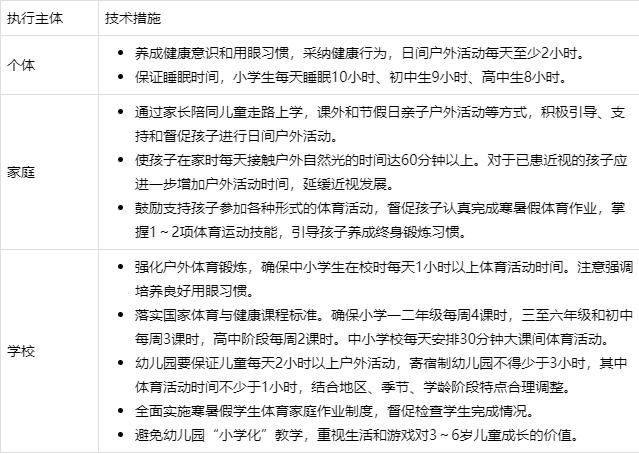
(E) Increase daytime outdoor activities.
Schools, families, and communities work together to reduce children and adolescents' long-term close-up work and provide related conditions for outdoor activities to encourage them.
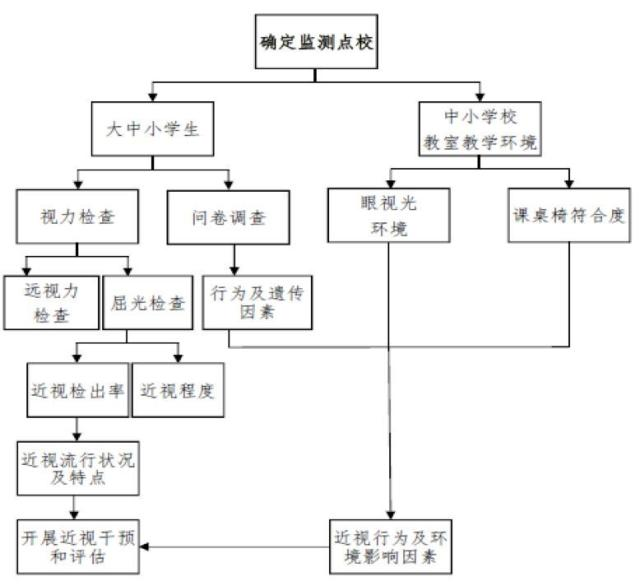
(F) Standardize vision health monitoring and evaluation.
Vision health monitoring and evaluation can promptly understand the distribution characteristics and trend changes of poor vision and myopia in student groups, determine high-risk groups and factors, and provide data basis for formulating and evaluating myopia prevention and control measures.
Develop local monitoring and implementation plans for common diseases and health influencing factors among students, organize relevant training, and carry out on-site investigations and monitoring, data entry, result analysis, and reporting. See Figure 3 for the myopia monitoring process.
Write myopia monitoring and evaluation reports at each level, report the reports to the government in a timely manner and inform the education administration department. Based on the local situation, formulate or adjust myopia intervention measures and activities, and publicize the main information to the society through the media.
(G) Scientific Diagnosis and Treatment.
After nearsightedness screening and monitoring, children and adolescents should be classified and managed according to their condition and receive scientific treatment.
1.For students with normal vision but with high-risk factors for myopia, it is recommended to change their high-risk behaviors and improve their visual environment.
2.For those with insufficient farsightedness reserves or decreased naked eye vision, their visual function may be abnormal. It is recommended to go to medical institutions for optometric examinations to make a clear diagnosis and take timely measures for correction.
3.Wearing frame glasses is the preferred method for correcting refractive errors. Parents are advised to go to medical institutions to choose suitable glasses for their children according to the requirements of doctors or optometrists, and to wear glasses as prescribed. For those with normal vision wearing glasses, preschool children should have their naked eye vision and wearing glasses vision checked every 3 months or 6 months, and primary and secondary school students should have them checked every 6 to 12 months. If the wearing glasses vision decreases, it is necessary to determine whether to replace the glasses under the guidance of a doctor.
4.For nearsighted children and adolescents who use low-concentration atropine or wear corneal reshaping lenses (OK lenses) to slow down the progression of myopia, it is recommended to go to regular medical institutions and follow the doctor's instructions.
Source: National Health Commission of the People's Republic of China website.

【Scan and follow us】




